In the 1980’s extracorporeal shockwave therapy was introduced for treatment of kidney stone disease and rapidly became the standard of therapy. Energy levels required to break up renal calculi were high and in the range of 90Mpa (Figure 1, Dornier MedTech Systems Wessling, Germany).
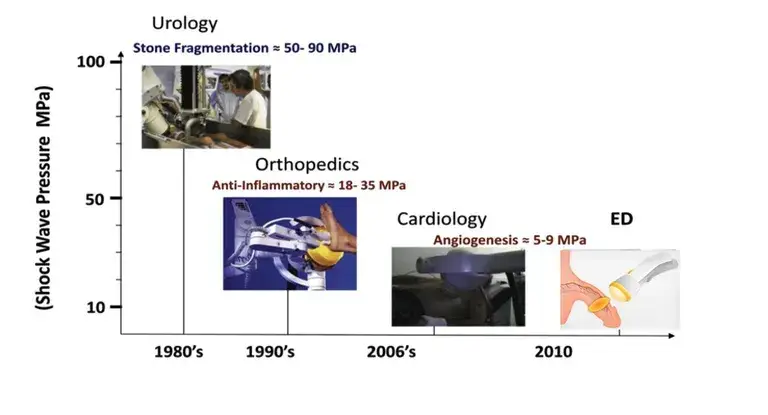
In 2010 Vardi et al first showed in a pilot study significant improvement in men with vasculogenic erectile dysfunction (ED) treated with low-intensity shockwave lithotripsy (LiST) using a energy of approximately 10Mpa. He then published in 2012 a randomized, double-blind, sham controlled study) again demonstrating significant improvement in erectile function in men treated with LiST. Since then LiST has gained popularity for the treatment of erectile dysfunction (ED) both internationally and in the United States. This has been bolstered by several high-quality and randomized studies supporting LiST’s efficacy in treating ED, and in some cases reversing ED. LiST presently does not have FDA clearance for use in the management of erectile dysfunction, penile curvature, penile pain, pelvic pain or low testosterone and is considered an off-label use of the various marketed devices.
ion this page I will present what we know about LiST. In particular, I will discuss what it is, what we know about how it works and its potential use in a number of men’s health issues. Following this I will discuss the device and protocol I use, the evaluation I perform prior to beginning treatment and the risks and potential benefits. If you are interested in finding out more please contact us to set up a courtesy consultation.
Low intensity extracorporeal (i.e., outside the body) shockwave therapy (LiST) is a treatment that has been in use since 2010 and has become commonly used Internationally and in the United States since 2015. Patients are usually treated in the office setting once or twice a week for 4 to 10 weeks. The device applies a low-intensity shockwave to the surface of the penis using an ultrasound gel as the coupling agent. LiST appears to have minimal side effects and is well-tolerated without any anesthesia. However, it has not received U.S. Food and Drug Administration (FDA) approval for treatment of erectile dysfunction, penile curvature, penile pain or low testosterone. It has received FDA approval for the treatment of plantar fasciitis, lateral epicondylitis and diabetic foot ulcers. The device I use, the Urogold 100 MTS, has been FDA cleared for improved blood flow, pain amelioration, connective tissue activation, wound healing and is considered a device with a non-significant risk to humans. Most of the current research with LiST for men’s health issues has been directed towards erectile dysfunction. A few studies have evaluated the use of LI-SWT for penile curvature, prostatitis and low testosterone. This article will primarily address the use of LI-SWT in the treatment of erectile dysfunction with occasional reference to the other treatments. I will add to this page as additional good studies becomes available.
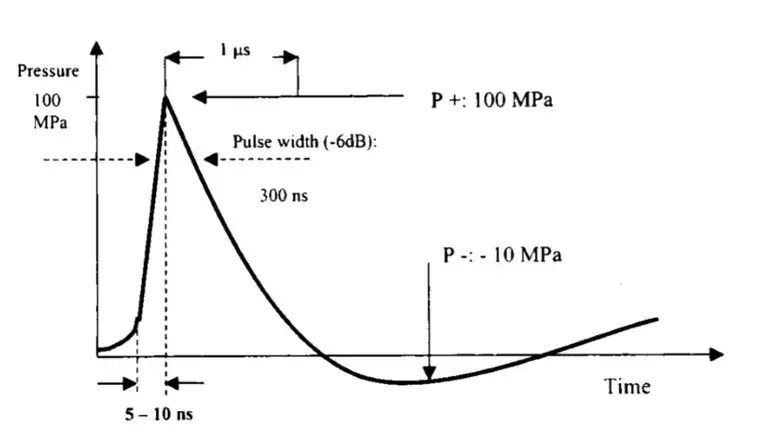
A shockwave is a single acoustic wave with a wide frequency range (150kHz up to 100 MHz), high pressure amplitude (up to 150mPa), low tensile wave (up to -25 MPa), small pulse width and short rise time (few hundred nanosecond) (Figure 2).
There are three types of shockwave generators manufactured and in use (Figure 3). Each if these devices produce a shockwave as described above and are considered a Class 2 medical device by the FDA and require premarket clinical safety and effectiveness data for approval by the FDA for each indication they apply for.
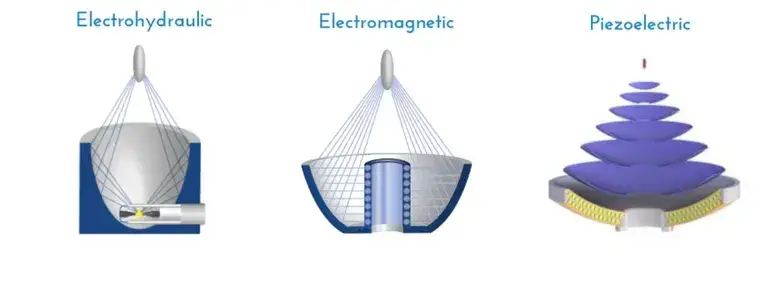
1. Electrohydraulic Generator – a voltage applied to an electrode immersed in water vaporizes water generating a shockwave.
2. Electromagnetic Generator – a voltage across metallic membranes produces a magnetic field causes an abrupt movement in a metallic membrane producing a shockwave
3. Piezoelectric Generator – a voltage applied to ceramic elements submerged in a medium expand producing a mechanical disturbance in the medium and a shockwave.
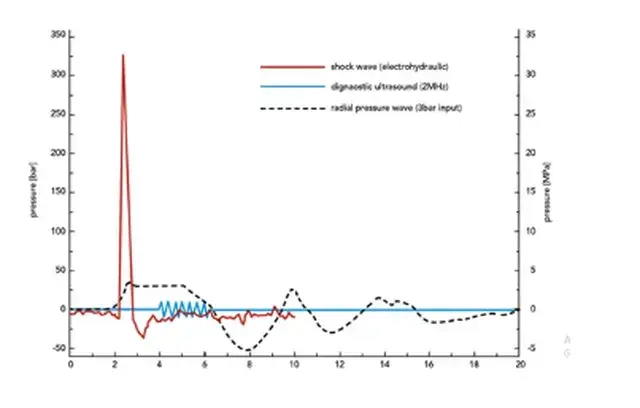
You should be aware that a device widely marketed in the United States uses a ballistic radial wave. In this device a controlled explosion of compressed air bursts a projectile into a probe creating a wave. These are not shockwave devices. The radial wave has a lower peak pressure, a slower rise time and propagate outward when compared to shockwaves (Figure 4). Radial waves also suffer from a greater loss of pressure at the interface between the probe and the penile skin surface. It is a Class 1 exempt medical device which does not require FDA clearance for use. Radial wave devices are commonly claimed to be “shockwave” devices however, as shown in Figure 4, they do not produce a wave with the characteristics of a shockwave. They also do not have clinical safety and effectiveness data nor are there published randomized clinical trials using these devices. Therefore, no statements can be made about the effectiveness of ballistic radial wave devices in the treatment of men’s health issues.
In comparing radial waves and shockwaves there is another important concept that needs to be considered. That of energy flux density (EFD). EFD is related to the energy of the shockwave (E), wave pressure (p), Area of the wave surface (A), Density of the medium, propagation speed in the fluid (c) and time (t)
Given by the formula: EFD = [E-A] =[1-pc] p2(t)dt
Of importance for use in treatment of men’s health issues is that with the radial wave device the maximal energy flux density (EFD) is reached at the tip of the applicator as compared with shockwave generators in which the maximal EFD is reached at a point (F2) inside the treated tissue (Figure 5).
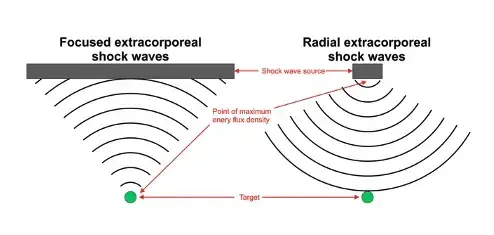
What this means practically, is that a radial wave generator has a maximum pressure that is 100 times lower than that of a shockwave generator. Also, the pulse durations are 1,000 times longer and the EFD and depth of penetration are lower. The ability of radial wave devices to supply energy to the penile cavernosal bodies which is required for the therapeutic effect as discussed above is therefore unknown. Until acceptable randomized controlled studies are done these devices are not recommended for use.
It is not completely understood how LiST works. However, the current theory is that the shockwave produced by the device causes stress on cell-membranes and release of growth factors and recruitment of stem cells that promote the development of new penile arteries and reduce inflammatory and cellular stress. In animal studies, there is also evidence to suggest there is nerve regeneration (Figure 6). LiST is unique in that it could provide a treatment option that corrects the underlying problem instead of just treating the symptoms. In the case of erectile dysfunction it is thought to be able to reverse the underlying vascular or neurogenic cause.
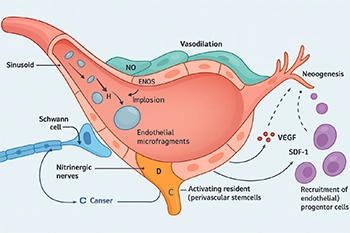
Figure 6: Putative mechanisms of action of shockwave therapy for ED. Shockwaves form microbubbles (A) in the vasculature and tissue that collapse (B) and cause disruption of the endothelium (C). Endothelial disruption might activate resident stem cells (D) and result in chemokine production with attraction of (endothelial) progenitor cells (E) and release of VEGF (F); these factors combine to initiate neoangiogenesis (G). In addition, microbubble collapse induces shear stress and might simulate endothelial NO production (H). Furthermore, shockwave therapy might also enhance Schwann- cell-mediated nitrergic-nerve repair after injury (I). Fode,M et al.Low-intensity shockwave therapy for erectile dysfunction: is the evidence strong enough? Nat Rev Urol 14, nrurol.2017.119 (2017).
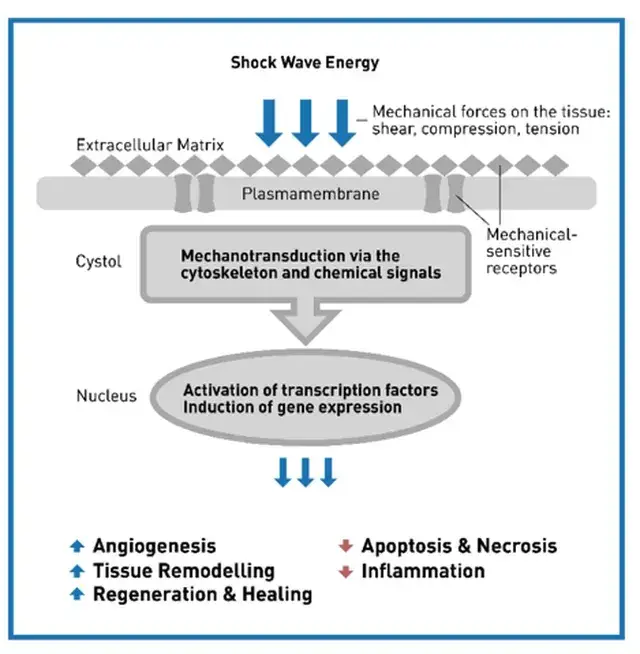
Specifically, as shown in Figure 6 and Figure 7, physical energy produced by the shockwave results in a mechanical stimulation to the cell and transduced int various cellular responses:
– The expression and release of regeneration-associated molecules is activated.
– Growth factors and signaling molecules (chemokines and cytokines) such as the vascular endothelial growth factor (VEGF), the vasodilator nitric oxide (NO), the proliferating cell nuclear antigen (PCNA), adenosine triphosphate (ATP), the stromal derived factor-1 (SDF), the fibroblast growth factor (FGF-.), the insulin-like growth factor (IGF-1), interleukins and many others which are released.
All these factors trigger intracellular signaling cascades which are implicated in processes like metabolic activation, proliferation, migration and recruitment of mesenchymal and hematopoietic progenitor cells, appears to result in improved angiogenesis, cavernous nerve cell regeneration and remodeling of cavernous stromal tissue. However, much work is still needed, some of which is underway, to elucidate and define the precise mechanism of action in urologic disease as well as to identify how often LiST is given, the number of shocks given per treatment and overall, the EFD used, duration of improvement and need for maintenance therapy. The answering of these questions is complicated by the number of shockwave devices in use and the different protocols used on each machine.
Please note: LiST presently does not have FDA clearance for use in the management of erectile dysfunction, penile curvature, penile pain, pelvic pain or low testosterone and is considered an off-label use. The device I use, the Urogold 100 MTS, has been FDA cleared for improved blood flow, pain amelioration, connective tissue activation, wound healing and is considered a device with a non-significant risk to humans. However, the device is being used ‘off-label’ for any of these men’s health issues.
1. Erectile Dysfunction
Regenerative therapies including low-intensity shockwave therapy, plasma rich plasma and stem cell therapy have generated a great deal of interest since 2015. However, low-intensity shockwave therapy has the most literature supporting its use.
20% of all men have erectile dysfunction (ED) with men of increasing age being disproportionally affected. The incidence of ED can be as high as 60% in men with Diabetes or cardiovascular disease. Although previously considered a quality-of-life issue, the presence of erectile dysfunction in an otherwise healthy man is now considered a harbinger of cardiovascular disease. Vascular factors are the leading cause of ED. A multitude of treatment options exists for those men with minimal or moderate erectile dysfunction, including pills, injections, external devices and surgical options. Unfortunately, these don’t work for every man and may interact with medications or underlying diseases. Also, they treat the symptoms and not the underlying cause of ED. LiST offers a potential treatment that can ameliorate the dysfunction and offer the potential to restore erectile function.
Several reviews of studies evaluating the use of LI-SWT have been published recently. The first was an analysis of ten randomized controlled studies completed over two years by Sokolakis and Hatzichristodoulou (Int Jour Impot Res, 31:177-194, 2019) which concluded that LiST significantly improved erectile function in patients with vascular ED. All ten studies used a validated questionnaire as the assessment tool and included men with moderate to severe ED. Their analysis also contained only 873 studies followed for less than one year. Three studies also measured penile hemodynamics.
A second systematic review by Brunckhorst et al. (Int Urol Neph, 51:773-781, 2019) reviewed eleven studies with 799 patients. Nine studies found an improvement in ED at six months after treatment with the improvement remaining above baseline out to 12 months.
A third review included seven randomized controlled studies evaluating the effect of LiST on erectile function (Dong et al., Am J Men’s Health, March-April:1-14, 2019). Evaluating outcomes by validated questionnaires (ie., International Index of Erectile Function – erectile function domain [IIEF-EF] and the Erectile Hardness Score [EHS]) they found improvement in erectile function after treatment with LiST.
Although the results have been encouraging, there are still many questions to be answered. What patients will respond to LI-SWT? Will the patients with worse erectile dysfunction, Diabetes and/or heart disease respond better or worse? Does patient age or use of oral or injectable medications used to treat erectile dysfunction affect the results of LI-SWT? What are the contraindications for the use of LI-SWT? Should we be treating men on blood thinners? How does the frequency and length of treatments affect the results? Is it better to use fewer treatments/week over a longer period of time? How does the intensity and number of shocks affect the outcome? Does the type of device matter (linear vs. focused shockwaves)? Focused shockwaves have shown their effectiveness while the results of linear shockwaves are still conflicting. When do the effects of LI-SWT occur and how long does the improvement last? These, among other questions, will need to be answered
Current literature demonstrates an improvement of erectile dysfunction with LiST. However, large, multicentered, randomized controlled studies which include not only qualitative (e.g. validated questionnaires) but also quantitative data (e.g. spectral ultrasound vascular data) are needed before LI-SWT becomes the standard of care.
2. Penile curvature and penile pain
The use of LiST for penile curvature (aka Peyronie’s disease) actually began 10 years earlier than that for treatment of erectile dysfunction. The literature for this indication is not as robust. A very nice review by Porst was recently published (Porst, H. Sex Medicine Rev 9, 93–122 (2020)). As Porst describes, the number of papers reviewed in the three published meta-analyses were limited. However, nine case-controlled studies and three randomized studies essentially came to the same conclusion that ‘LiST may be an effective and safe treatment for reducing penile plaque size and relieving pain but not for improving penile curvature’.
The design of these studies also presented a challenge on interpreting the data as it has been in the literature on ED. Porst noted that the disparity in these studies regarding the energies used, shockwave machines employed, number of shocks per session and total number of shocks given was even greater than that in the literature for ED. Obviously much more work is needed.
3. Prostatitis, Pelvic pain and Low Testosterone
There is limited literature available on the use of LiST for Prostatitis, Pelvic pain and Low Testosterone. However, this is currently an area of active investigation.
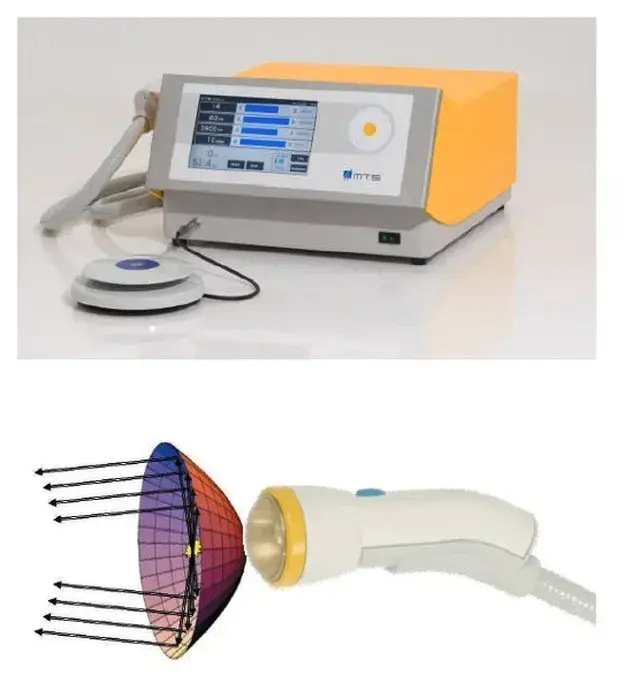
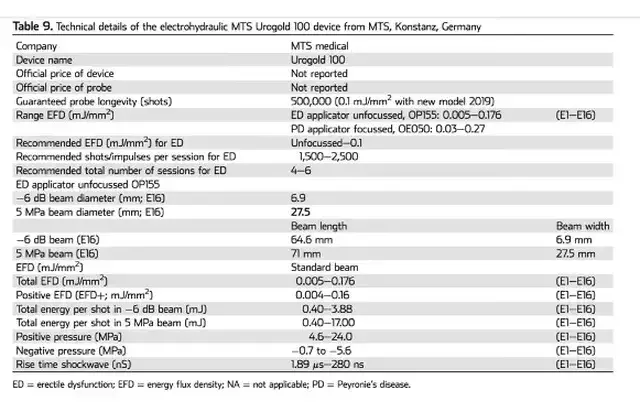
The device I use, the Urogold 100 MTS (Figure 8; upper panel) , is an electrohydraulic device that has been FDA cleared for improved blood flow, pain amelioration, connective tissue activation, wound healing and is considered a device with a non-significant risk to humans. It does not have specific FDA clearance for use in the management of erectile dysfunction, penile curvature, penile pain, pelvic pain or low testosterone and use for these conditions it is considered off-label. The device has a parabolic unfocused applicator. The generated shockwave energy is reflected into a parallel collimated beam which provides for less pain and a wider surface of energy then focused probes (Figure 8; lower panel) (https://www.mts-medical.com/en_US/produkte/urologie/urogold100/)
The energy flux density used is between 0.05 and 0.16 mJ/mm2. The full technical specifications for the device are listed in the table below:
Our protocol
Prior to consideration of treatment with LiST I discuss with each prospective patient their goals and expectations. I also explain the relative risks and potential benefits of the treatment. I obtain a complete medical history and require several questionnaires to be completed.
There are absolute and relative contraindications for treatment with LiST. Patients with absolute contraindications will not be treated with LiST.
Absolute contraindications for LiST treatment for urologic conditions include:
1. Patients with pacemakers or implantable defibrillators.
2. Patients who are using devices which are sensitive to electromagnetic radiation.
3. Patients with urologic cancer.
4. Patients with severe coagulation disorders.
5. Patients younger than 18 years of age.
Relative contraindications for LiST treatment for urologic conditions include:
1. Patients being treated with anticoagulants.
1. Of note: There are two randomized studies with men on anticoagulants or antiplatelet therapy (Kalyvianakis, D et al, J Sex Medicine (2019)). “In these studies 138 patients were included in the 2 trials, whereas 135 (98%) of them finished the 3 months follow-up. 35 (25.3%) of them were under anticoagulant/antiplatelet medication during LiST. No bleeding events or any other side effects were reported.”
There is also baseline testing that we require prior to beginning therapy. I have listed these below. There are also questionnaires and testing performed after completion of treatment to assess outcome known as endpoints. These will be evaluated prior to treatment, 3, 6, 12 and 24 months after treatment.
A) Questionnaires and Validated Instruments
1. International Index of Erectile Function (IIEF)
2. Erectile Hardness Score (EHS)
3. Men’s Health Questionnaire
B) Ultrasound parameters:
1. Peak PSV
2. Average penile firmness on elastography (Kpa)
C) Maximal penile tumescence and rigidity with pharmacologic agent
D) Penile length: flaccid, stretched and stimulated
E) Penile girth
We will also obtain blood studies prior to treatment. These blood tests will include:
1. Hormonal studies: Testosterone, LH, FSH
2. CBC with platelets
3. PTT,PT/INR
4. Metabolic profile
5. Lipid panel
Treatment can begin at the completion of the above requirements and signing of an informed consent
1. Shockwave therapy may be given in either a flaccid or in an erect phallus after a pharmacologic injection
2. The shockwave is applied to several areas of the phallus as well as the perineum
3. Usually six treatments are given. The spacing between treatments is discussed with the patient at the beginning of the treatments. Treatments can be given:
1. Once a week for two weeks and then every other week thereafter. A total of 6 treatments are given over a 10-week period.
2. Once a week for six weeks.
3. Twice a week for three consecutive weeks
4. Three times a week for two consecutive weeks
4. Post treatment evaluation, questionnaires and ultrasound studies are begun at 12 weeks measured from the date of the first treatment
The Urogold 100 MTS is considered by the FDA to be a device with a non-significant risk to humans. In a phase 2 study (Patel et al. Sex Med, 8, 214–222, 2020) investigating the safety of LiST. They randomized patients into two Groups. Group A received once a day treatment over 5 consecutive days (Monday to Friday), in which 720 shocks of LiST were applied in every session, half to each treated region (left and right corpora cavernosa and crura). Group B consisted of once a day 3 sessions per week (Monday, Wednesday, and Friday) for 2 consecutive weeks, in which 600 shocks of LiST were applied. No immediate side effects of erythema, pain or swelling have been noted with LiST treatment for ED. Not every patient noted an improvement in erectile function. In a phase 2 trial 8% of men noted a worsening of their erectile function on a validated questionnaire (IIEF). In this same study no scar, plaque or penile deformity was noted at six to 12 months. They concluded that LiST can be used safely for the treatment of erectile dysfunction by trained and knowledgeable providers.
For questions please contact my office at 516-487-2700 or email (FrontDesk@nycryo.com)
Additional Reading:
1.Yih, J., Minton, J., Gagnon, C. & Goldstein, I. 009 Retrospective Chart Review of Treatment Outcome Following Low-Intensity Shockwave Therapy for the Treatment of Vestibulodynia with Urogold 100TM MTS. J Sex Medicine 17, S4–S5 (2020).
2.Yih, J. 195 Retrospective Chart Review of Treatment Outcome Following Low-Intensity Shockwave Therapy for the Treatment of Vestibulodynia with Urogold 100TM. J Sex Medicine 17, S67–S68 (2020).
3.Yih, J., Goldstein, S., Georgeon, L., Ramirez, R. & Goldstein, I. 318 Retrospective Review of Improvement of Erectile Function after Low Intensity Shockwave Treatment with Urogold 100TM. J Sex Medicine 17, S78 (2020).
4.Chung, E. et al. Clinical Practice Guideline Recommendation on the Use of Low Intensity Extracorporeal Shockwave Therapy and Low Intensity Pulsed Ultrasound Shockwave Therapy to Treat Erectile Dysfunction: The Asia-Pacific Society for Sexual Medicine Position Statement. World J Men’s Heal 38, (2020).
5.Yih*, J., Minton, J., Gagnon, C., Goldstein, S. & Goldstein, I. PD36-10 LUMBO-SACRAL LOW INTENSITY SHOCKWAVE THERAPY FOR GENITO-PELVIC DYSESTHESIA/PERSISTENT GENITAL AROUSAL DISORDER (GPD/PGAD) USING UROGOLD 100 MTS. J Urology 203, e726–e727 (2020).
6.Patel, P. et al. Phase II Randomized, Clinical Trial Evaluating 2 Schedules of Low-Intensity Shockwave Therapy for the Treatment of Erectile Dysfunction. Sex Med-uk 8, 214–222 (2020).
7.Porst, H. Review of the Current Status of Low Intensity Extracorporeal Shockwave Therapy (Li-ESWT) in Erectile Dysfunction (ED), Peyronie’s Disease (PD), and Sexual Rehabilitation After Radical Prostatectomy With Special Focus on Technical Aspects of the Different Marketed ESWT Devices Including Personal Experiences in 350 Patients. Sex Medicine Rev 9, 93–122 (2020).
8.Brunckhorst, O. et al. A systematic review of the long-term efficacy of low-intensity shockwave therapy for vasculogenic erectile dysfunction. Int Urol Nephrol 51, 773–781 (2019).
9.Liu, T., Shindel, A. W., Lin, G. & Lue, T. F. Cellular signaling pathways modulated by low-intensity extracorporeal shockwave therapy. Int J Impot Res 31, 170–176 (2019).
10.Sokolakis, I. & Hatzichristodoulou, G. Clinical studies on low intensity extracorporeal shockwave therapy for erectile dysfunction: a systematic review and meta-analysis of randomised controlled trials. Int J Impot Res 31, 177–194 (2019).
11.Vita, R., Benvenga, S., Giammusso, B. & Vignera, S. L. Determinants of Early Response to Low-Intensity Extracorporeal Shockwaves for the Treatment of Vasculogenic Erectile Dysfunction: An Open-Label, Prospective Study. J Clin Medicine 8, 1017 (2019).
12.Dong, L. et al. Effect of Low-Intensity Extracorporeal Shockwave on the Treatment of Erectile Dysfunction: A Systematic Review and Meta-Analysis. Am J Men’s Heal 13, 1557988319846749 (2019).
13.Mauro, M. di et al. Extracorporeal Shockwave Therapy in Peyronie’s Disease: Clinical Efficacy and Safety from a Single-Arm Observational Study. World J Men’s Heal 37, (2019).
14.Mortensen, J., Ladegaard, P. B. J., Skov-Jeppesen, S. M. & Lund, L. HP-09-005 A prospective randomized placebo controlled study evaluating the combined effect of Low-intensity Extracorporeal Shockwave Therapy (LI-ESWT) and vacuum erectile device on Peyronies Disease. The Journal of Sexual Medicine 16, S47–S48 (2019).
15.Usta, M. F., Gabrielson, A. T. & Bivalacqua, T. J. Low-intensity extracorporeal shockwave therapy in the treatment of erectile dysfunction following radical prostatectomy: a critical review. Int J Impot Res 31, 231–238 (2019).
16.Wang, C.-J., Lu, Y.-M., Li, C.-C., Wu, W.-J. & Chien, T.-M. Low-intensity shockwave therapy ameliorates erectile dysfunction in men with pelvic fractures associated with urethral injury. Int J Impot Res 31, 218–222 (2019).
17.Capogrosso, P. et al. Low-Intensity Shockwave Therapy in Sexual Medicine—Clinical Recommendations from the European Society of Sexual Medicine (ESSM). J Sex Medicine 16, 1490–1505 (2019).
18.Kalyvianakis, D., Memmos, D., Mykoniatis, I., Kapoteli, P. & Hatzichristou, D. Low-Intensity Shockwave Therapy (LiST) for Erectile Dysfunction: Is It Safe for Patients on Anticoagulant Medication? J Sex Medicine(2019) doi:10.1016/j.jsxm.2019.05.008.
19.Yamaçake, K. G. R. et al. Low-intensity shockwave therapy for erectile dysfunction in kidney transplant recipients. A prospective, randomized, double blinded, sham-controlled study with evaluation by penile Doppler ultrasonography. Int J Impot Res 31, 195–203 (2019).
20.Campbell, J. D. et al. Meta-analysis of randomized controlled trials that assess the efficacy of low-intensity shockwave therapy for the treatment of erectile dysfunction. Ther Adv Urology 11, 1756287219838364 (2019).
21.Krieger, J. R., Rizk, P. J., Kohn, T. P. & Pastuszak, A. Shockwave Therapy in the Treatment of Peyronie’s Disease. Sex Medicine Rev (2019) doi:10.1016/j.sxmr.2019.02.001.
22.Katz, J. E., Clavijo, R. I., Rizk, P. & Ramasamy, R. The Basic Physics of Waves, Soundwaves, and Shockwaves for Erectile Dysfunction. Sex Medicine Rev 8, 100–105 (2019).
23.Fode, M., Russo, G. I. & Verze, P. Therapeutic areas of Li-ESWT in sexual medicine other than erectile dysfunction. Int J Impot Res 31, 223–230 (2019).
24.Mousa, R. A. et al. [50] The efficacy and safety of low-intensity shockwave therapy in erectile dysfunction. Arab J Urology 16, S25 (2018).
25.Li, P.-C. et al. [Low-intensity extracorporeal shockwave therapy for Peyronie’s disease: A preliminary study of 32 cases]. Zhonghua nan ke xue = National journal of andrology 24, 340–344 (2018).
26.Li, X. et al. Comparative effectiveness of extracorporeal shockwave, ultrasound, low-level laser therapy, noninvasive interactive neurostimulation, and pulsed radiofrequency treatment for treating plantar fasciitis. Medicine 97, e12819 (2018).
27.Zewin, T. S. et al. Efficacy and safety of low-intensity shockwave therapy in penile rehabilitation post nerve-sparing radical cystoprostatectomy: a randomized controlled trial. Int Urol Nephrol 50, 2007–2014 (2018).
28.Zou, Z., Liang, J., Liu, Z., Gao, R. & Lu, Y. Low-intensity extracorporeal shockwave therapy for erectile dysfunction after radical prostatectomy: a review of preclinical studies. Int J Impot Res 30, 1–7 (2018).
29.Man, L. & Li, G. Low-intensity Extracorporeal Shockwave Therapy for Erectile Dysfunction: A Systematic Review and Meta-analysis. Urology 119, 97–103 (2018).
30.Rizk, P. J., Krieger, J. R., Kohn, T. P. & Pastuszak, A. W. Low-Intensity Shockwave Therapy for Erectile Dysfunction. Sex Medicine Rev (2018) doi:10.1016/j.sxmr.2018.01.002.
31.Ruan, Y. et al. The effect of low‐intensity extracorporeal shockwave therapy in an obesity‐associated erectile dysfunction rat model. Bju Int 122, 133–142 (2018).
32.Fojecki, G. L., Tiessen, S. & Osther, P. J. S. Effect of Linear Low-Intensity Extracorporeal Shockwave Therapy for Erectile Dysfunction—12-Month Follow-Up of a Randomized, Double-Blinded, Sham-Controlled Study. Sex Med-uk 6, 1–7 (2017).
33.Fojecki, G. L., Tiessen, S. & Osther, P. J. S. Effect of Low-Energy Linear Shockwave Therapy on Erectile Dysfunction—A Double-Blinded, Sham-Controlled, Randomized Clinical Trial. J Sex Medicine 14, 106–112 (2017).
34.Clavijo, R. I., Kohn, T. P., Kohn, J. R. & Ramasamy, R. Effects of Low-Intensity Extracorporeal Shockwave Therapy on Erectile Dysfunction: A Systematic Review and Meta-Analysis. J Sex Medicine 14, 27 35 (2017).
35.Angulo, J. C. et al. Efficacy of low-intensity shockwave therapy for erectile dysfunction: A systematic review and meta-analysis. Actas Urológicas Españolas Engl Ed 41, 479–490 (2017).
36.Lin, G. et al. In Situ Activation of Penile Progenitor Cells With Low-Intensity Extracorporeal Shockwave Therapy. J Sex Medicine 14, 493–501 (2017).
37.Korneyev, I. A. et al. Low intensity shockwave therapy for erectile dysfunction: 6 months followup results. Urologicheskie Vedomosti 7, 5–13 (2017).
38.Inoue, S. et al. Low-intensity extracorporeal shockwave therapy for patients with severe erectile dysfunction due to radical prostatectomy. Ann Res Hosp 1, 2–2 (2017).
39.Lu, Z. et al. Low-intensity Extracorporeal Shockwave Treatment Improves Erectile Function: A Systematic Review and Meta-analysis. Eur Urol 71, 223–233 (2017).
40.Tsai, C.-C. et al. Low-Intensity Extracorporeal Shockwave Therapy Can Improve Erectile Function in Patients Who Failed to Respond to Phosphodiesterase Type 5 Inhibitors. Am J Men’s Heal 11, 1781–1790 (2017).
41.Fode, M., Lowenstein, L. & Reisman, Y. Low-Intensity Extracorporeal Shockwave Therapy in Sexual Medicine: A Questionnaire-Based Assessment of Knowledge, Clinical Practice Patterns, and Attitudes in Sexual Medicine Practitioners. Sexual Medicine 5, e94–e98 (2017).
42.Stoykov, B. A. et al. Low-Intensity Extracorporeal Shockwave Therapy – A New Approach in the Treatment of Erectile Dysfunction after Radical Prostatectomy. J Biomed Clin Res 10, 104–110 (2017).
43.Group, Y. A. U. M. H. et al. Low-intensity shockwave therapy for erectile dysfunction: is the evidence strong enough? Nat Rev Urol 14, nrurol.2017.119 (2017).
44.Kalyvianakis, D. & Hatzichristou, D. Low-Intensity Shockwave Therapy Improves Hemodynamic Parameters in Patients With Vasculogenic Erectile Dysfunction: A Triplex Ultrasonography-Based Sham-Controlled Trial. J Sex Medicine 14, 891–897 (2017).
45.Chung, E. PS-07-012 Analysis of predictors for clinical success and patient satisfaction rate following low intensity shockwave therapy in men with erectile dysfunction and Peyronie’s disease: A prospective open-label single arm study. J Sex Medicine 14, e130–e131 (2017).
46.Pan, M. M., Raees, A. & Kovac, J. R. Low-Intensity Extracorporeal Shockwave as a Novel Treatment for Erectile Dysfunction. Am J Men’s Heal 10, 146–148 (2016).
47.Kitrey, N. D. et al. Penile Low Intensity Shockwave Treatment is Able to Shift PDE5i Nonresponders to Responders: A Double-Blind, Sham Controlled Study. J Urology 195, 1550–1555 (2016).
48.Xin, Z.-C. AB067. Future ED therapy: low-energy shockwave therapy and low-intensity pulsed ultrasound therapy. Transl Androl Urology 4, AB067 (2015).
49.Olsen, A. B., Persiani, M., Boie, S., Hanna, M. & Lund, L. Can low-intensity extracorporeal shockwave therapy improve erectile dysfunction? A prospective, randomized, double-blind, placebo-controlled study. Scand J Urol 49, 329 333 (2015).
50.Chung, E. & Cartmill, R. Evaluation of clinical efficacy, safety and patient satisfaction rate after low‐intensity extracorporeal shockwave therapy for the treatment of male erectile dysfunction: an Australian first open‐label single‐arm prospective clinical trial. Bju Int 115, 46 49 (2015).